Benign breast conditions information provided by Breast Cancer Now
WHAT IS LOBULAR NEOPLASIA?
Lobular neoplasia is a benign (not cancer) condition.
Breasts are made up of lobules (milk- producing glands) and ducts (tubes that carry milk to the nipple). These are surrounded by tissue that gives breasts their size and shape.
The breast
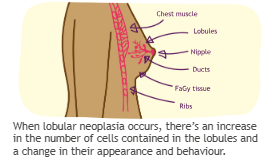
When lobular neoplasia occurs, there’s an increase in the number of cells contained in the lobules and a change in their appearance and behaviour.
TYPES OF LOBULAR NEOPLASIA
There are different types of lobular neoplasia.
These are:
- Atypical lobular hyperplasia (ALH)
- Classical lobular carcinoma in situ (LCIS)
- Pleomorphic lobular carcinoma in situ (PLCIS)
‘In situ’ means the changes only occur in the breast lobules and do not affect the surrounding breast tissue.
When tissue is examined under a microscope, ALH and classical LCIS can look very similar.
Call our Helpline on 0808 800 6000
It’s sometimes difficult to separate the two conditions and they may both be described as lobular neoplasia.
PLCIS is made up of larger, more abnormal cells.
WHO IT AFFECTS
Lobular neoplasia is most common in women aged 40–50, but it can be found in women of any age.
It can be found in men, but this is extremely rare.
DIAGNOSING LOBULAR NEOPLASIA
Lobular neoplasia doesn’t usually cause any symptoms or show up on a mammogram.
It’s usually found during a biopsy or other test being done for another breast change. For example, when calcifications (small spots of calcium) are detected on a mammogram.
If lobular neoplasia is found by a core biopsy, your specialist may recommend removing more tissue from the area where the lobular neoplasia was found. This is to check if there are any cancer cells in this part of the breast.
This may be done using one of the following:
- Core biopsy – using a hollow needle to take a sample of tissue, under local anaesthetic, to be looked at under a microscope (several tissue samples may be taken at the same time)
- Vacuum assisted excision biopsy – a hollow probe connected to a vacuum is used to take a sample of tissue, under local anaesthetic, to be looked at under a microscope
- Excision biopsy – a sample of breast tissue is removed and looked at under a microscope. An excision biopsy can be carried out under a local or general anaesthetic.
You can find out more about these tests in
our booklet Your breast clinic appointment.
A mammogram or ultrasound scan may also be used to help identify the area. Your
treatment team will talk to you about which procedure is best for you.
TREATING LOBULAR NEOPLASIA
ALH and LCIS
You will not usually need treatment for ALH and classical LCIS, but your specialist may discuss treatment options with you based on current guidelines and your individual situation.
PLCIS
If the biopsy shows PLCIS, your specialist may suggest an operation to remove the area with a margin (border) of healthy breast tissue.
This is because of the higher risk of breast cancer with this type of lobular neoplasia. The operation will show if there are any cancer cells in the tissue, and if all the PLCIS has been removed.PLCIS is often treated in the same way as ductal carcinoma in situ (DCIS), which is a type of early breast cancer. Radiotherapy or hormone therapy may be recommended. You can find more information about DCIS in our Ductal carcinoma in situ (DCIS) booklet.
Depending on your individual situation, some specialists may recommend hormone therapy to treat ALH, classical LCIS and PLCIS (see ‘Hormone therapy’).
DOES LOBULAR NEOPLASIA INCREASE MY RISK OF BREAST CANCER?
Most women diagnosed with ALH or classical LCIS will never get breast cancer. However, there is a slightly higher risk than the general population of developing breast cancer in either breast.
Women diagnosed with PLCIS are more at risk of developing breast cancer than those with ALH or classical LCIS.
Your individual risk depends on several factors, which your specialist can discuss with you.
Hormone therapy
Research has shown that treating women who have lobular neoplasia with tamoxifen (a hormone therapy treatment for breast cancer) can reduce the risk of breast cancer developing.
However, any possible benefit of taking tamoxifen needs to be considered against the risks and side effects of this treatment. Your specialist will discuss this with you if this might be an option.
See our Tamoxifen booklet for more information.
Visit breastcancernow.org
FOLLOW-UP
Your specialist will usually recommend having yearly follow-up mammograms for up to five years.
If you have other risk factors for breast cancer, such as a significant family history, scans may be recommended, such as an MRI (magnetic resonance imaging) scan. Your specialist will discuss which follow-up is best for you.
You can find out more about family history onour website breastcancernow.org
Hormone replacement therapy (HRT) HRT and oral contraceptives are not usually recommended for people after a diagnosis of lobular neoplasia.
FURTHER SUPPORT
Finding out that you have lobular neoplasia can leave you feeling different emotions.
Fear, shock and anger are all common feelings. Although lobular neoplasia is not breast cancer, it can cause uncertainty about your future risk of breast cancer and you may feel anxious.If you’re worried about breast cancer or have a question about lobular neoplasia, our specialist team are ready to listen. Call our free Helpline on 0808 800 6000.
ABOUT THIS LEAFLET
Lobular neoplasia was wriGen by Breast Cancer Now’s clinical specialists, and reviewed by
healthcare professionals and people affected by breast conditions.
For a full list of the sources we used to research it: Email
health-info@breastcancernow.org
You can order or download more copies from
breastcancernow.org/publications
We welcome your feedback on this publication:
health-info@breastcancernow.org
For a large print, Braille
or audio CD version: Email
health-info@breastcancernow.org
Medical disclaimer
We make every effort to ensure that our health information is accurate and up to date, but it doesn’t replace the information and support from professionals in your healthcare team. So far as is permiGed by law, Breast Cancer Now doesn’t accept liability in relation to the use of any information contained in this publication, or third-party information included or referred to in it
©Breast Cancer Now, June 2022. All rights reserved BCC126, Edition 5, next planned review 2025
Breast Cancer Now is a company limited by guarantee registered in England (9347608) and a charity registered in England and Wales (1160558), Scotland (SC045584) and Isle of Man (1200). Registered Office: Fifth Floor, Ibex House, 42–47 Minories, London EC3N 1DY.
CHECKING YOUR BREASTS IS AS EASY AS TLC
TOUCH YOUR BREASTS
Can you feel anything new or unusual?
LOOK FOR CHANGES
Does anything look different to you?
CHECK ANY NEW OR UNUSUAL CHANGES WITH A GP
Breast cancer is most common in women over 50. While uncommon, it can also affect younger women.
Men can also get breast cancer, but this is very rare.
Get into the habit of regularly checking your breasts.
WE’RE HERE FOR YOU
We want everyone to have the confidence to check their breasts and report any new or unusual changes.
If you have any questions or worries about your breasts or breast cancer, call us free and confidentially.
0808 800 6000